




The light is fading on a late Thursday afternoon in December. In a small workspace on Cordova Street, a group of men sit casually around a table, trading stories about fentanyl, the powerful opioid that has caused a record-breaking spike in B.C. overdose deaths.
“I have a friend who gets those fentanyl patches. He cooks ’em down and takes the fentanyl off the patches and dries it up. He cooks about two of ’em. He gives me some, and I say, ‘You better watch it man, that stuff’s very potent,’” says Lee Gladue, 53. “He gives me 60 units. Fentanyl didn’t do nothing for me!”
Kevin Thompson, 46, nods. “My first couple times doing it, I felt nothing,” he says. “I’m like, ‘What are these guys saying, they’re high? They’re just boxed out of their minds. And I felt nothing.’”
As an illicit drug overdose crisis gripped British Columbia, killing 914 people last year, fentanyl was often portrayed as a demon drug.
Dean Wilson, a longtime harm reduction advocate and former heroin user, wants to set the record straight. “There’s nothing wrong with fentanyl. Fentanyl’s just another opiate,” he says. It has been widely used to manage pain in the health care system.
The problem, he says, is fentanyl’s unregulated presence in the illicit drug market.
“The real issue is that we just don’t know what’s in it, in the drugs we’re purchasing,” he says. The unknown potency of illicit drugs, and the fact drugs are often cut with other substances — in B.C., street fentanyl shows up in opioids like heroin and also stimulants like cocaine and methamphetamine — is what can lead to fatal overdoses, he adds.
Wilson says two things need to happen to address the overdose crisis. “One, either allow us to test our drugs, or two, give us the drug,” he says.
“Start moving on the injectable hydromorphone. Let’s get moving on the injectable diacetylmorphine. Let’s get going on this stuff,” Wilson says, referring to European therapies that include providing long-term users with injectable opiates that have only been used with two Vancouver patients outside of clinical trials. “Because that’s the only way to actually solve the problem.”

Wilson’s call for a clean supply of drugs runs counter to the mainstream public discussion about the opioid crisis.
“There’s a lot of drug war rhetoric: ‘police have to stop this from coming in; we have to get to the Chinese; we have to clamp down,’” says Canadian Drug Policy Coalition director Donald MacPherson. (The B.C. government has been concerned about China because of its lack of regulations around fentanyl.)
Fentanyl, he says, is just the latest in a long line of drugs that capture the spotlight and distract people from the simpler truths about drug use and drug policy.
“We really need to acknowledge that drug use exists,” he says. “Fentanyl is a product of our drug policies. What prohibition does is it encourages the criminals to move highly concentrated drugs… the fentanyl war on drugs is going to drive more prohibition, which in turn is going to just keep creating the same-old, same-old problem: uncontrolled, illegal drugs of unknown strengths, toxic drugs. Drugs that are mixed with all sorts of shit.”
Ending the drug hustle
The demon fentanyl didn’t seem to have an effect on Gladue and Thompson. They are longtime, high-tolerance drug users, previously entrenched in illicit opioid addictions that left space for little else in their lives.
Gladue says he turned to heroin when his doctor cut him off from a morphine prescription on the Sunshine Coast before he realized he was addicted. He came to the Downtown Eastside for heroin “just to get better,” he says. “That’s how I ended up staying down here… I’m not going to stand up there and get sick.”
The violent, humiliating illness that characterizes opioid withdrawal — symptoms include fevers, chills, shakes, intense nausea, vomiting and incontinence — can keep people in drug addiction.
But for Gladue, Thompson and nearly 150 of their peers who have previously battled long-term illicit opioid addiction, the threat of illness related to withdrawal is now gone.
They’re receiving precisely what Wilson and MacPherson are calling for — a clean, crime-free supply of the drugs.
Every day, Gladue, Thompson and others on the program go to Vancouver’s Crosstown Clinic, where medical staff supervise as they inject themselves with a pharmaceutically prepared dose of diacetylmorphine (pharmaceutical-grade heroin which, since September 2016, physicians can now request through Health Canada’s Special Access Programme or hydromorphone (a more widely accessible opioid analgesic sold in Canada under the brand name Dilaudid).
Crosstown patients go to the clinic for scheduled doses two to three times a day. Dosages vary and are measured to meet individuals’ needs, which can change over time. Participants are also free to change their treatment plan, move towards an abstinence-based model or leave the program anytime. While they’re at Crosstown, they also have access to other health care and social services from physicians, nurses and social workers.
This is the Injectable Opioid Assisted Treatment Program (iOAT), an outgrowth of the SALOME clinical trial, which ran at Crosstown from December 2011 to late 2015. Short for Study to Assess Long-term Opioid Maintenance Effectiveness, SALOME tested alternative treatments for people with chronic addiction and for whom other available treatments, like methadone, were not working.
SALOME was a Vancouver trial that built upon the success of its predecessor, the North American Opiate Medication Initiative (NAOMI). The groundbreaking heroin-assisted treatment clinical trial ran in Vancouver and Montreal from 2005 to 2008 with 251 participants. Like the SALOME participants, NAOMI participants also had access to social workers, nurses, and physicians to assist them with aspects of life beyond drug addiction.
Thompson was part of both NAOMI and SALOME, and continues to access services through iOAT. He says the program was instrumental to turning his life around.
“Boom. All the help came to me from there,” Thompson says. “They got me housing… I’m actually stable enough that I started working. I got employed. I quit crime.” He says he’s had no police encounters for over seven years — a long time for a person who was shoplifting to survive.
Before he joined NAOMI in his mid-thirties, Thompson was homeless and sleeping on the sidewalk on Cordova Street, near where he now lives in social housing in the Woodward’s building. He shoplifted to support an addiction to crack and cocaine.
Coming down after three days of cocaine (research has shown that many younger people who are homeless use stimulants to stay alert and keep themselves safe), Thompson would snort a line of heroin to manage his cocaine withdrawal, typically characterized by depression, anxiety and feeling run down.
One day, he thought he was coming down with the flu, but he remembers his dealer telling him, “No, you’re wired [addicted to heroin]. [He] threw me a paper. I did it. And wow,” Thompson says, referring to a hit of heroin. His symptoms were gone, and he felt normal. “That’s day one when I knew I was wired.”
He kept shoplifting to buy more heroin. “I was just chasing to be un-sick,” Thompson says. “I hated being sick. ’Til you’re a heroin addict, you’ll never know what it feels like to wake up sick like that… you’re so edgy that you just want it out… that’s the worst feeling to me.”
Thompson was living on the street when he met Kurt Lock, a health research coordinator who was recruiting drug users to participate in NAOMI. After participating in that program, he moved on to SALOME, where a social worker helped him find a spot in social housing in the nearby Woodward’s complex. “I’d been on BC Housing’s list for 12 years,” he says.
Today, Thompson works as a supervisor at the newly opened overdose prevention unit at the Washington Needle Depot a few blocks from where he lives.
“This is a big step,” he says. Working with people during the opioid overdose crisis, he thinks about what would happen if he were still on the streets, buying from dealers instead of getting medication in a clinical, decriminalized setting.
“I’d be a statistic, I guarantee you,” he says. “My habit was so out of control. I probably wouldn’t be here today.”

Not one overdose death
Providence Health Care’s Crosstown Clinic has been a pivotal force in the Downtown Eastside community.
“There are people using at Crosstown Clinic that I know from Insite,” says Ronnie Grigg, who has worked overnight shifts as a mental health worker at the Insite supervised injection facility for almost eight years.
Their lives have been transformed by the clinic’s program providing drugs and support.
“When I run into them on the street, they are in a far better place. Removing the stress of the street hustle, which can be sex trade, a lot of it is theft, property theft, or violence… remove those additions, and that is inherently is transformative. And it’s transformative for the community as well.”
Grigg is run ragged from working back-to-back overnight shifts through the fentanyl crisis at Insite, where staff members are increasingly being asked by community members to attend overdoses happening on surrounding sidewalks and alleyways. “It’s a little more than the average person signed up for, to be running to emergencies in the lanes and sidewalks.”
The Downtown Eastside has suffered mightily, losing many of its residents to opioid overdoses. Earlier this month, the Vancouver Area Network of Drug Users and former Vancouver East MP Libby Davies called on the BC Coroners Service to release the names of Downtown Eastside community members who have died to begin the process of healing.
For participants in Crosstown’s program, it’s a different story. “Our patients in this clinic have sort of been inoculated,” says Dr. Scott MacDonald, the physician lead for the Providence Crosstown Clinic. “Maybe it’s our treatment approach, I don’t know. But we’re just not seeing the consequences of the opioid crisis — other than we think that there’s a treatment that works, and if it was more widely available, we think the crisis would not be having the impact that it is.”
Of the almost 150 people in the iOAT program at Crosstown, no one has died from an overdose. MacDonald also sees other benefits. “It reduces the load on emergency medical services. It reduces criminal justice system costs. It reduces policing costs. It reduces judiciary system costs. It reduces incarceration costs,” he says.
MacDonald would like to see opioid-assisted treatments like those on offer at Crosstown expanded to meet the needs of the relatively small number of people who require such treatments. “I know there’s 500 people in Vancouver, including the 150 that we’re already treating, that do [opioid assisted] treatment,” he says.
“There’s about 16,000 to 17,000 people on opioid substitution treatment in British Columbia. So I would predict that the number of people in British Columbia who would need an intensified treatment like this to be in the area of 1,000 or so. That is not a huge number. That is a number that British Columbia could meet.” (About 15,000 people in B.C. are on methadone maintenance programs; some 2,000 are on suboxone to rapidly reduce withdrawal symptoms.)

Public supports legalized drugs
We seem to have both the public support and political will to make such treatments more widely available.
In late November 2016, the Mustel Group polled 500 B.C. residents over the phone about their thoughts on legalizing hard drugs in response to the opioid crisis.
The survey, commissioned by the Vancouver mental health and addictions non-profit InnerChange Foundation, found 93 per cent of respondents supported making drug counselling and psycho-social care — therapy that considers psychological factors and the social environment — available to address overdoses and addictions.
Seventy-seven per cent supported more opioid substitution programs like NAOMI, SALOME, and iOAT.
B.C. Health Minister Terry Lake defended NAOMI and SALOME when the Harper government banned the use of opiate-substitution medications in 2013.
“If they didn’t have the names of those drugs, we would just call them medicine and we would use them,” Lake says. “It’s the way you approach it that’s important. If the end goal is to keep people healthier, to reduce disease, mortality, morbidity, and if you can help people get on a better path, then to me, that’s medicine.”
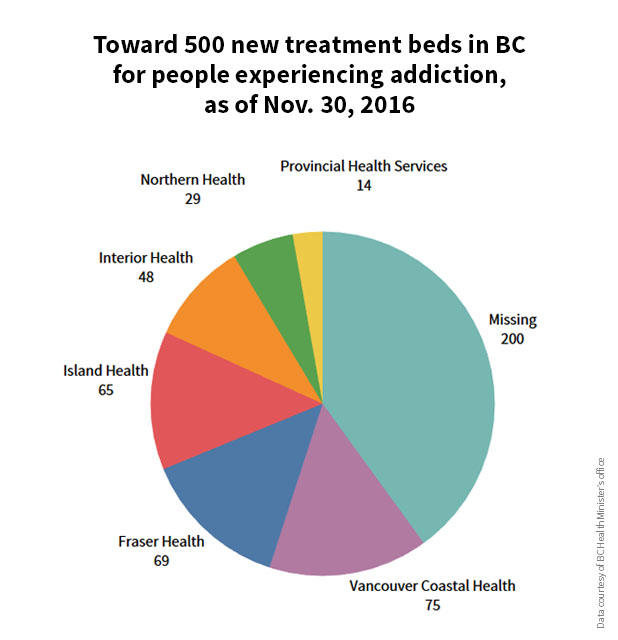
Lake has promised to open 500 more treatment beds across the province by the end of March. Last week, he announced that the province would also open 50 intensive outpatient therapy beds, plus 60 publicly funded residential treatment beds. Those publicly funded treatment beds, he said, would put up to 240 people a year through a 90-day treatment program.
“Both these beds and outpatient treatment spaces will target those who are most vulnerable and who are ready to seek treatment,” he told reporters.
At the same time, he says the government will invest more in mental health and substance use.
“That’s going through the budgeting process for 2017-18,” he told me in December. “I think there’s a growing recognition, not just in B.C. but across the country, that we need to invest more in mental health and substance use. But it’s difficult because the emergency room, and the hip replacement, the knee replacement, they capture people’s attention. And it’s challenging to divert resources from one area into another area. So we have to be thoughtful about how we do it. And we have to have a long-term plan. So it’s difficult to do overnight without impacting other areas of the health care system.”
No room in a program that could save lives
At the same press conference where the coroner announced the death toll for 2016 last week, Provincial Health Officer Dr. Perry Kendall told reporters that while B.C. is expanding access to conventional treatment programs, it’s not the answer for some people.
Those people need programs where legal substitutes for heroin and other street drugs are provided, he said. Programs like the one on offer through the Crosstown Clinic, and which are part of the healthcare system in the Netherlands, Switzerland, Germany, Denmark, and the United Kingdom.
“These treatment, while very controversial in North America, are proven to work,” Kendall said. “Like methadone and suboxone [oral opiate substitues], they improve physical and mental health and social functioning. They’re cost-effective and take people out of illegal drug markets.” He noted the need to evaluate the potential for such treatments to reach more people in Canada. But “that’s down the road,” he said.
Meanwhile, people eager to begin those treatment programs today are shut out.
“On a regular basis I have people coming to my office begging to get into the Crosstown Clinic because they know the participants from SALOME and can see how well they are doing,” says Kurt Lock, research co-ordinator for the Centre for Health Evaluation and Outcome Sciences which, in partnership with Providence Health Care, ran NAOMI, SALOME and now iOAT.
It’s not easy to manage their disappointment, he says. “I tell them that the government and the health authorities are working on it, but the truth is that as of December, there are no concrete plans to expand the treatment, in Vancouver anyways. The unfairness that their peers who made it through the SALOME window and are getting this government-funded, life-saving treatment makes the conversation especially difficult and upsetting.”
Community members know their peers in iOAT are living free of the worries that consume their own lives, Lock says. They aren’t worried about overdosing, or getting sick from opioid withdrawal. “It is tragic that in light of the current overdose crisis, that the provincial government and health authorities are not moving faster to expand the treatment offered at the Crosstown Clinic when it could do so much to save lives.”
The iOAT participants are living with fewer burdens now than they have for years. But they also carry a degree of survivor’s guilt.
“Just the amount of my friends who’ve died just this year, I could fill half of my wall at home with just pictures [of them]. [More pictures] than the last 25 years of my life,” says Kevin Thompson. “I’ve got friends who are dying to get into this program. I hope they do before they become a statistic.”
The day I talked to Thompson, Dec. 15, 13 people died of drug overdoses. Nine lived in Vancouver.
Last in the series: Solutions from Blood Reserve, where a fentanyl epidemic struck in 2014, plus a first look at a pioneering opioid addiction therapy in progress in Vancouver. ![]()
Read more: Health











Tyee Commenting Guidelines
Comments that violate guidelines risk being deleted, and violations may result in a temporary or permanent user ban. Maintain the spirit of good conversation to stay in the discussion.
*Please note The Tyee is not a forum for spreading misinformation about COVID-19, denying its existence or minimizing its risk to public health.
Do:
Do not: