




For weeks now, Medicine Hat emergency room physician Dr. Paul Parks has been warning the public about what he asserts is a looming crisis in Alberta’s health-care system, a crisis he says will overwhelm the province’s already over-capacity and understaffed hospitals and lead to unnecessary deaths.
Almost daily on social media, Parks has bluntly stated that Alberta's health-care system is now so dysfunctional and chaotic that it will be unable to handle the inevitable surge of sick patients from the annual flu, respiratory infection and COVID season over the next few months.
As a recent former president of the Alberta Medical Association and during his 25 years as an ER doctor, Parks has been an outspoken critic of the political meddling in, and mismanagement of, Alberta's health-care system.
Parks knows there are many, especially within Premier Danielle Smith’s United Conservative Party government, who will accuse him of being hyperbolic.
“I hate being the voice and advocate out here that is trying to alert Albertans and say, ‘Hey, we should pay attention. Things are bad,’” said Parks on a recent episode of the podcast The Breakdown.
“But bad doesn't cut it. It is pure chaos. I have used that word a lot, and people are like, ‘Is it hyperbole? Am I exaggerating here?’
“No. It has never been this chaotic and this difficult to navigate, and it has never been this overcrowded. It has never been this bad.”
The worst is yet to come, said Parks, who told The Tyee he is planning a series of town halls across Alberta to raise awareness.
Parks is not alone in his assessment.
The Tyee has obtained — not from Parks — internal Alberta health graphs from various presentations, including some to the government. Independent health policy experts who reviewed the graphs at The Tyee’s request say they clearly support the warnings now being issued by Parks.
“I know Paul Parks and he is not given to overstatement,” said Dr. James Talbot, Alberta's chief medical officer of health from 2012 to 2015 and a sharp critic of the current government’s health policies.
Talbot said the chances of a crisis in Alberta’s health-care system are “unfortunately good” and he anticipates “a lot of pressure on hospitals from pretty much November through to February.”
‘They have created the perfect storm’
Both Talbot and University of Calgary health law professor Lorian Hardcastle directly blame what they say are the ill-informed and ill-timed policies of the UCP government for the looming crisis.
“They have created the perfect storm of factors that led to this poorly performing, toxic health-care system,” Hardcastle said. “And all of that would be bad enough any time of the year, but it is especially bad going into respiratory virus season.”
Primary and Preventative Health Services Minister Adriana LaGrange and Hospital and Surgical Health Services Minister Matt Jones did not respond to a request for comment from The Tyee about whether they think a crisis is looming, and if so, what, if anything, they are doing to prevent it.
In July, LaGrange’s ministry told CBC that “a clear, phased plan is guiding how the system will operate” and that “transformation of this scale takes time, but progress is well underway.”
There are three major factors that form the “perfect storm” that Hardcastle referenced.
The first is that the province’s major hospitals are already at, or over, capacity, which means there are now not enough beds for patients.
The second is that the government decided to undertake a total — and what many health policy experts have said is an unnecessary — dismantling and reconstruction of Alberta Health Services, or AHS, the province’s massive health-care service provider. And the government undertook this “disintegration” directly after a pandemic that left many staff exhausted and burned out.
The third factor is the province’s low immunization rate, which health policy experts blame on the Smith government's ideological decision to not promote flu, COVID and respiratory vaccines and to not widely distribute and pay for them.
Alberta’s biggest hospitals over capacity
In an email, Parks said all the current health-study literature states that hospitals should aim for 85 per cent maximum occupancy of beds to be functional and efficient, and to allow for volume variations. Efficiency falls drastically with occupancy over 90 per cent; over 100 per cent produces gridlock.
An internal Alberta Health Services graphic shows a current average occupancy rate of 101 per cent. Hospitals in Red Deer, Calgary and Edmonton range from 105 per cent to a high of 113 per cent at Calgary’s South Health Campus. The smaller regional hospitals are all hovering around 90 per cent.
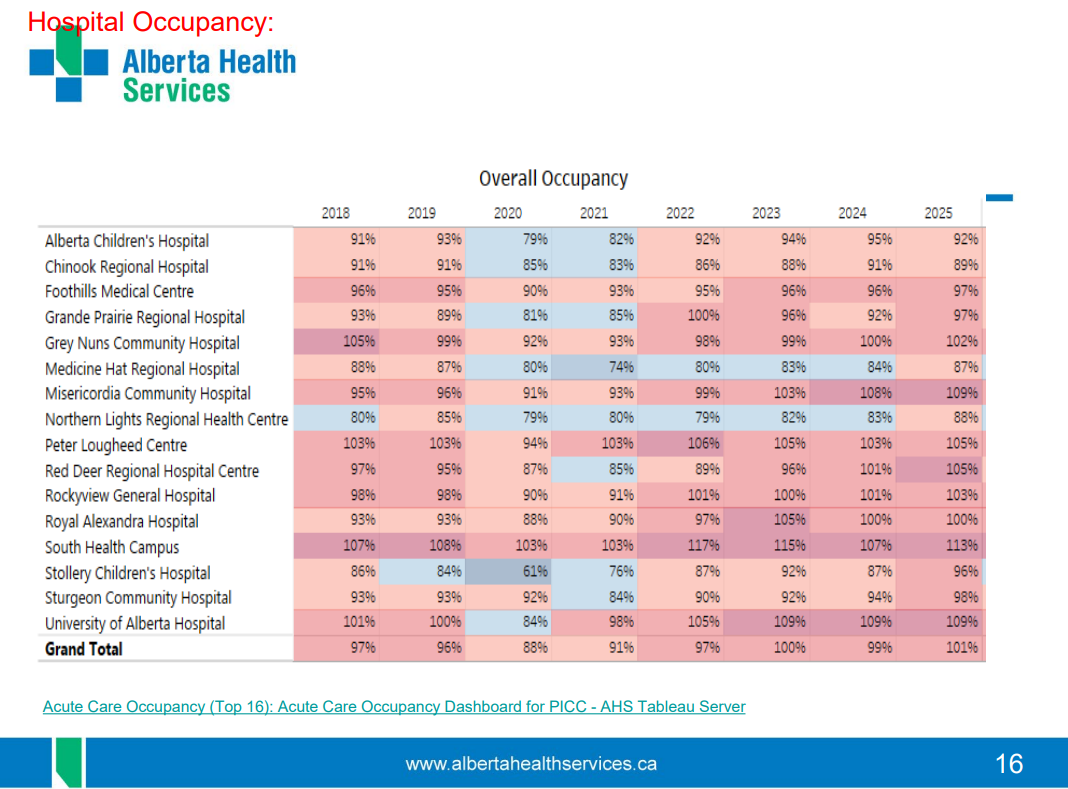
Talbot said that when a hospital is over 100 per cent capacity, people are being treated in hallways or in suboptimal rooms.
It means people who are brought into emergency with a broken hip or leg may wait on a hallway stretcher for several days before they get surgery. And it means people with other various ailments may wait 12 hours or more to be seen.
Parks was also the section lead for the province’s emergency room doctors and still regularly talks with colleagues across the province.
He told The Breakdown that, for example, the emergency room at the University of Alberta Hospital in Edmonton sometimes has 60 care spaces, “and there will be 70, 80, 90, 100 patients out in the waiting room, waiting to go in.”
“There are sometimes 60 admitted patients that need to be [admitted] who should be up on the floors. Sixty out of 60, every one on a stretcher, is someone with a stroke or someone that needs surgery, or someone that has had a horrible heart attack and needs to go to specialized care.
“And there is no space to care for anybody, and the ambulances keep coming.”
Another slide shows that a troubling percentage of those who walk into the emergency room, and even some brought in by ambulance, leave without being seen.
The problem is worst in Edmonton, where 21 per cent of patients left Edmonton’s Royal Alexandra Hospital, the main hospital for northern Alberta and the inner city, without being seen. Red Deer also has a serious problem with 15.9 per cent of patients giving up and leaving.
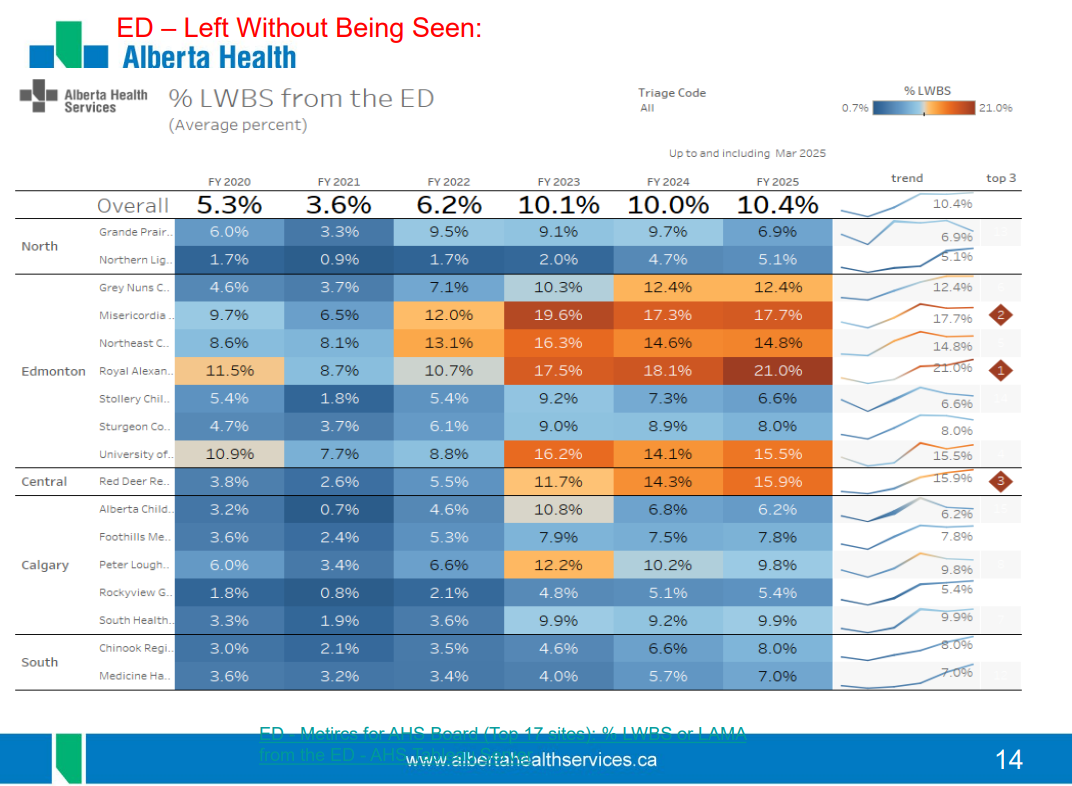
Talbot calls that a “deadly statistic” because people who leave often return “in a much worse state, more likely to require hospitalization, more likely to require an ICU [intensive care unit] bed, more likely to have a bad outcome, like dying.”
Parks said he knows of cases where people have tried to sign themselves out to go to another hospital, including a case in which a patient had waited seven days to get their broken hip fixed.
A main cause of insufficient beds is patients known in health-care parlance as “bed blockers” — mostly elderly people who should be in an alternate level of care, or ALC, such as long-term care facilities or home support.
A confidential internal Alberta Health document obtained by The Tyee shows that about 40 per cent of the beds at Sturgeon Community Hospital in St. Albert and nearly 37 per cent of the beds at Misericordia Community Hospital in west Edmonton are taken up by ALC patients.
Calgary’s South Health Campus and Rockyview General have 20.6 and 20.3 per cent, respectively, of beds filled with ALC patients.
A ‘byzantine’ major restructuring
During the provincial election, Danielle Smith promised to lay the groundwork for fixing Alberta’s health-care system within 90 days. It has taken far longer than that, but the UCP government has nonetheless undertaken a blitzkrieg dismantling of a health-care system that was once the fifth most integrated in the world.
Smith had publicly complained that AHS had too many administrative staff and not enough frontline workers.
Since the reorganization was announced in November 2023, thousands of AHS staff have been transferred to four new health agencies: Acute Care Alberta, Primary Care Alberta, Recovery Alberta and Assisted Living Alberta.
Each of the four new agencies is overseen by a minister and a newly created attendant bureaucracy.
Several more organizations are being created to individually manage emergency services and other services such as organ donation and transplantation. Five health zones will be replaced by seven health corridors and somehow, at some point, decision-making will be decentralized to the hospital level.
Critics like Talbot and Parks question how this exponential increase in bureaucracy will reduce administrative staff.
Every health policy expert interviewed by The Tyee said they have no idea why the UCP government would blow up the former system instead of applying targeted fixes, nor why they chose to do it directly after a pandemic that nearly overwhelmed the health-care system.
Steven Lewis is a Vancouver-based health policy expert who has worked extensively as a consultant and academic in various Canadian provinces, including Alberta. He is unaware of any other jurisdiction that has implemented a pillared or siloed system like the one in Alberta.
Every health-care system has units or subdivisions, Lewis said, but they are generally integrated with singular leadership and governance. In contrast, Alberta has created a system with separate “pillars,” each with its own CEO, minister and layers of bureaucracy.
“Which is what you would create if you aimed for disintegration. And this obvious reality creates the need for yet another structure to co-ordinate the parts, but it is unclear what the co-ordinating mechanism does,” he said.
“Many people will need services across two or even all four pillars. Who controls the budgets for cross-pillar services?”
“The whole structure is byzantine and highly original, but not in any rational way,” Lewis said.
‘Why are we doing this?’
Parks is more blunt in his assessment. The four agencies, he said, are “fully disconnected,” and there is “zero integration, zero operational control.”
Hardcastle, the University of Calgary health law policy expert, said the reorganization made no sense from the outset.
“If you look back to when the reorganization was announced, there was a resounding ‘Why are we doing this?’ from experts who research health policy.”
Parks said he has never heard a frontline worker suggest the system needed to be blown up and rebuilt in a bunch of disconnected pieces.
“Where this came from is still a mystery. I would love for the premier to tell us who came up with this and what experts said this would be a good idea,” he said.
“For the last two years, they have been trying to push a square peg into a round hole, when everybody on every front has been saying, ‘This is not working.’”
Hardcastle said the timing of the implosion of AHS also made no sense.
“Our system was not in a position where it was ready for organizational chaos when it had not yet recovered from COVID,” she said. “This is an inopportune time to be experimenting with a health system reorganization.”
The system needed stability. Instead, Smith fired the CEO, the entire AHS board and the chief medical officer of health, and senior management has been a “revolving door” for the past two years, Hardcastle said.
There are also multiple investigations underway, including a criminal investigation, and a wrongful-dismissal lawsuit related to allegations of massive procurement corruption within AHS.
Hardcastle said staff are still burned out from the pandemic and don’t want to be placed in a situation where they have to work large amounts of overtime while dealing with high patient-to-staff ratios.
“I don't know how much of that health-care workers can withstand at this point,” she said.
“If health-care workers had a better relationship with this government, they would perhaps be more tolerant of these kinds of pressures. But the toxic relationship that has persisted for a number of years now doesn't help that situation, and it doesn’t help recruitment and retention.”
Low immunization rates will stress hospitals
Parks and Talbot, the former chief medical officer of health, are unsurprised by the AHS graphic that charts seasonal respiratory hospital admissions. It shows what they say are highly predictable increases in patients attending ER and being admitted to hospital.
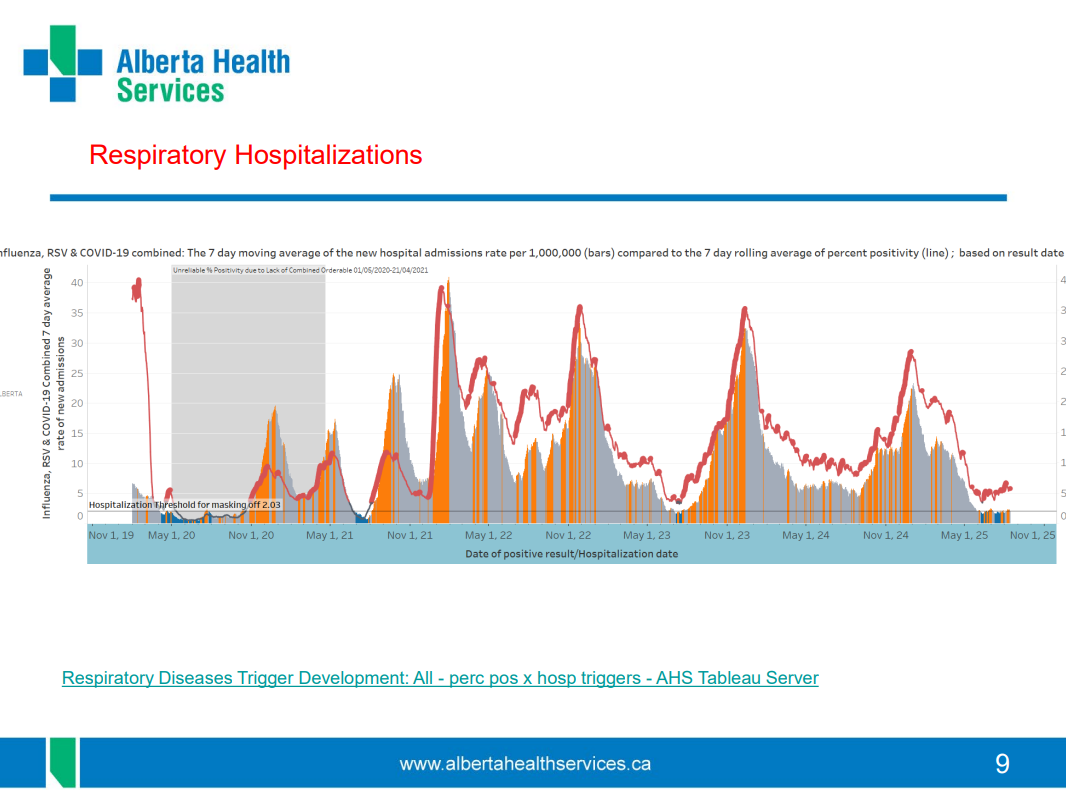
“We get spikes every fall and winter,” Parks said in an email. “Now we're going into the fall drastically overcrowded, and with all of our surge capacity used, that means we will be unable to accommodate the seasonal volumes we know are coming.”
The UCP government consciously decided not to adequately promote immunization, Talbot said. It has actively framed vaccinations as a personal choice. And it is not broadly distributing or paying for most Albertans to be vaccinated for flu, COVID or respiratory viruses.
It is, in total, a remarkably anti-scientific and counterproductive policy that will result in increased illness and death, Talbot said.
On Wednesday, Alberta Medical Association president Dr. Brian Wirzba issued a statement that contained an AMA analysis of the cost of the province’s low-immunization policy.
“If only five per cent of Albertans are deterred from getting vaccinated, the projected additional health-care costs exceed $65 million in hospitalization costs alone,” the letter states. “This far surpasses any savings the province might achieve through spending less on vaccines or minimizing wastage.”
The Smith government criticized AHS for not having enough beds to handle pandemic surge capacity in previous years. But Talbot said there is no health-care system in the world that can produce enough beds when immunization rates are low.
“One of the most inaccurate things that the government promotes is that deciding to get immunized is purely a personal choice,” he said.
“As we saw during COVID, when beds are totally occupied by people who were not immunized, surgeries have to be cancelled, cancer therapies have to be delayed, and there are potentially delays in people being seen in emergency departments that could result in very serious outcomes as well.
“Prevention is absolutely your first line of defence. It is your best line of defence. It is the most cost-effective line of defence. And a failure to do that proves that getting immunized is not just a personal decision.”
Talbot said that since the Smith government has decided it would accept low immunization rates as a health policy, basic human compassion should require it to invest in more continuing care beds, more acute care beds and greater emergency department capacity to handle the higher volumes.
But it has not.
In a mandate letter issued earlier this month, the premier directed Assisted Living Minister Jason Nixon to work with the minister of hospital and surgical health services “to commence the transition of non-acute patients in hospitals to alternative settings outside of the hospital that are more appropriate to their health status and needs.”
Talbot said the directive is too little, far too late.
The UCP government, he said, appears to have learned nothing from the pandemic’s lessons and is “prepared to gamble with a system that is less prepared than it was before COVID and in which they have invested less in prevention than they ever have before.”
“We are about to see how many people out there are not immunized or partially immunized, and if the virus spreads as it has in the past, there will be pressure in terms of the number of hospitalizations.
“Respiratory admissions in January and February, when COVID and influenza both tend to peak, is five times what it is at baseline. So you have to ask yourself whether this is a system that can handle a five-times increase.
“And the graphs that you have shows that it is not.”
If you have any information for this story, or information for another story, please contact Charles Rusnell in confidence via email. ![]()











Tyee Commenting Guidelines
Please note that email notifications for replies are not currently working due to a software issue which may be resolved in a future update.
Comments that violate guidelines risk being deleted, and violations may result in a temporary or permanent user ban. Maintain the spirit of good conversation to stay in the discussion and be patient with moderators. Comments are reviewed regularly but not in real time.
Do:
Do not: