



Kelowna psychiatrist Neil Hanon was at a medical conference in the United States two years ago when he got a text from one of his patients back home. The patient said he had tried to hang himself the night before.
Hanon turned to another psychiatrist at the conference, Phil Wolfson, a pioneer in the use of the anesthetic ketamine in therapy for mental illness such as treatment-resistant depression.
Hanon says Wolfson encouraged him to try ketamine with this patient.
“So, I went ahead with this fellow,” Hanon recounts, “and he went from acutely suicidal to cured. And I was like, ‘Oh my god.’”
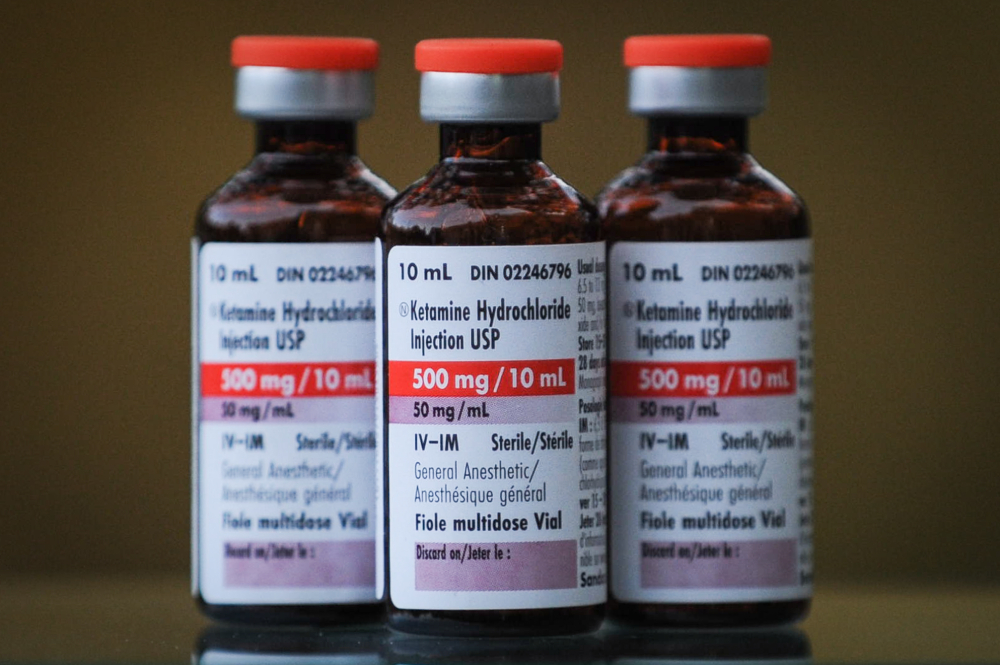
Hanon says that transformation took about four or five sessions. Each involved just a few millilitres of ketamine — about half a teaspoon — put under the patient’s tongue. Ten minutes or so after the dose, the drug would produce a psychedelic effect.
“You may see things. You may feel weird things,” Hanon says. “You still know who you are, you are in a non-ordinary state of consciousness. You’re able to see things differently about yourself. You don’t have the same fear responses.”
I immediately understand what Hanon means. I had several sessions of ketamine-assisted psychotherapy after I was diagnosed with severe post-traumatic stress disorder in 2014. In my case, it was an intramuscular dose of ketamine, injected into my thigh. My doctors who administered it helped me immensely. I would even say they saved my life. I did not interview them, nor did I seek their opinions for this story.
The loss of ego Hanon describes is temporary, but long enough for him to use talk therapy to help the patient work through what they previously couldn’t or wouldn’t see. The breakthroughs achieved in this augmented consciousness remain after the psychedelic effect wears off about an hour or two later.
A “cure” is by no means guaranteed. Most of Hanon’s patients who receive ketamine-assisted therapy at his private practice and the street clinic where he works get it regularly.
“I have one woman who has a ketamine session every two weeks,” Hanon says. “Her suicidality returns at about day 10. In an ideal world I would be giving her ketamine every 10 days — but I can’t.”
The reason? Hanon says the College of Physicians and Surgeons of B.C. won’t let him.
In March — without notice, publication or input from doctors using ketamine to treat mood disorders — the college unilaterally imposed a policy restricting what it calls a “novel” use of ketamine.
The college’s position statement prohibited anyone except an anesthetist from giving it to a patient, no matter how the drug is administered — either orally, intravenously or by injection into muscle.
What’s more, the college decreed ketamine can only be used in an “accredited non-hospital medical/surgical facility.”
The edict means that in order to use it, Hanon would have to set up the equivalent of a surgical centre and hire an anesthetist. The rules effectively bar any psychiatrist working out of a clinic — or from their home offices, as some do — from using a drug that’s cheap, effective, vastly improves lives and anecdotally at least, saves them.
“I was taught to help people,” Hanon says, looking back on three decades as a psychiatrist. “But the college has become Big Brother-ish, saying ‘No, if that’s not on label you can’t do that,' and it makes no sense to me.”
The college won’t say whether the issue is that Hanon and others are using ketamine “off label” — meaning as a treatment for which the drug wasn’t originally approved. The college declined a request for an interview.
There are plenty of examples of off-label drugs that have the college’s blessing — tacit or otherwise. For example, retinal specialists treating macular degeneration inject a colon cancer drug called Avastin into their patients’ eyes, instead of the drug Lucentis which is approved for the treatment, because it’s a fraction of the cost and effective. Quetiapine, approved to treat schizophrenia, is sometimes prescribed for people who have trouble sleeping.
Ketamine was developed as a powerful anesthetic more than half a century ago. In the 1970s, U.S. soldiers carried it with them into combat in Vietnam. The World Health Organization classifies ketamine as one of the safest and most essential drugs there is, in part because as a sedative it has a low risk of affecting respiration. Today it’s used in virtually every hospital and medical clinic, frequently in small doses, as a sedative.
In doses too small for anesthesia, ketamine behaves as a psychedelic. Decades ago, it gained notoriety as “Special K” — a party drug that can induce dissociation and amnesia when taken in large enough doses. It can be addictive. Abusers can build tolerance.
But the prescriptions written by doctors using ketamine in therapy are logged, tracked and available for instant review by the colleges of physicians and surgeons. Patients don’t take the drug home. It’s administered by the doctor in their office. And it works.
Randomized, placebo-controlled research as far back as 2000 confirmed ketamine — even without any therapy — produced significant antidepressant effects that lasted a week or longer. The first approved ketamine clinics opened in the U.S. in 2014. There are now scores that offer ketamine intravenously, not just for pain but for depression. A single treatment, without any therapy, can cost upwards of $800.
In Canada, a handful of clinics have begun to carve out a ketamine niche. One such place is Field Trip in Toronto. The clinic offers a course of sublingual ketamine — tablets placed under the tongue. The treatments are spread out over a few weeks. The cost is $4,700 and includes integration sessions which help patients learn from what they’ve experienced. None of it is covered by any public health insurance plan.
In contrast, Hanon’s work with patients is covered by the Medical Services Plan in B.C., and the cost of the ketamine he uses is less than $30 a dose.
Ontario psychiatrist Mark Cornfield has also used an inexpensive tablet form of ketamine in his practice.
“At low doses, ketamine is a lot like MDMA,” Cornfield says. “It’s relational. It takes your mask off. It’s an empathogen. It allows you to see your defences, and that you don’t need to use them. It’s an amazing lubricant at low doses for talk therapy.”
But just as Hanon and other doctors in B.C. discovered the provincial regulator effectively halted ketamine-assisted psychotherapy, Cornfield heard of a similar clampdown brewing in Ontario.
After months of inquiries, the College of Physicians and Surgeons of Ontario acknowledged to Cornfield that it had quietly struck an internal working group to determine which forms of ketamine for mood disorders should be restricted to hospital-like facilities employing anesthetists. Right now, Ontario doctors can still use oral and intranasal ketamine without those prohibitions, but Cornfield doesn’t know much longer that will be allowed.
Cornfield helped draft a formal letter to the college asking for a delay in any rule changes and a commitment to involve doctors who actually use ketamine for psychotherapy. More than 30 Ontario doctors signed it. Another 20, many from B.C., also put their names to the letter.
“The college is not our friend,” Cornfield said. “They’re rigid. They’re inflexible. They tend to be punitive. I can tell you most physicians, if they get a letter form the college, they start to shake in their boots.”
Cornfield is nearing the end of his career and so he persisted. After more prodding, the college eventually responded with a time-limited offer for ketamine providers: they had three weeks to send in their comments. No other involvement. No transparency about who is on the internal committee examining the rules, or what expertise those people have to evaluate ketamine-assisted therapy.
Cornfield says it makes little sense to form policy about a drug if you don’t rely on the people with experience using it.
“The people who control it are mostly anesthetists,” Cornfield says, referring to speculation by some that the restrictions are being influenced by the specialists who see ketamine as their domain. “[Anesthetists] have no idea about its use in mental health and have no concept of its relative safety, or lack of it, in subanesthetic doses. Even though at anesthetic doses it’s phenomenally safe.”
The apparent crackdown by regulators in Ontario and B.C. has also left some providers scratching their heads.
In July, Health Canada followed the U.S. Food and Drug Administration’s approval of Spravato, a ketamine-based nasal spray developed by Janssen Pharmaceuticals, a subsidiary of Johnson & Johnson.
Janssen developed its formulation after the patent on ketamine expired in 2002. That’s the reason why ketamine is relatively cheap: it’s a generic drug.
But Janssen did some research and found that a portion of the ketamine molecule called esketamine produced mood-altering qualities too. Janssen patented its derivative and received FDA approval for its use with treatment-resistant depression.
Spravato isn’t cheap. A couple of sprays every week for a month can cost thousands of dollars, without any therapy. Patients are expected to keep using it. It’s intended to augment — not replace — traditional antidepressants, which the colleges and many doctors appear unwilling to consider being in the same realm as psychedelics.
British psychiatrist David Healy has been an outspoken critic of the pharmaceutical industry and its relationship with doctors.
“We’ve created a monster,” Healy says about the proliferation of antidepressants. There are about three million people in the U.S. with what’s termed “treatment-resistant depression,” a phenomenon that didn’t exist before modern antidepressants.
Ketamine, Healy says, shows real promise.
“There’s convincing evidence that people who are severely depressed, that you can get these people well within days. The problem for the drug companies is they don’t really want you to get well in days, they want you to remain on treatment for years. So, the nasal version of ketamine is a much lower dose of ketamine that doesn’t get you well in days and costs a huge amount of money and you keep taking it for years.
“It’s not clear this is a good idea,” he adds.
The antidepressants Healy criticizes were born by accident in the 1950s when drugs that increased the level of serotonin in the brain appeared to generate a sense of euphoria in some patients. Since then, pharmaceutical companies have produced a dizzying array of drugs designed to alter the level of various neurotransmitters.
The mechanism by which this helps some sufferers — which today is still just theory — has been the subject of much skeptical scrutiny. Even those who embrace antidepressants acknowledge they are far from being as proven and efficacious as many would like to believe.
Igor Galynker is a professor of psychiatry at the Icahn School of Medicine at Mount Sinai in New York City and head of the Mount Sinai Beth Israel suicide research lab who has studied antidepressant use.
“In my experience, one out of five people will feel acutely better,” he said. “Three people feel like they have a thicker skin. And one person will feel worse.”
Here again, I know exactly what Galynker is talking about. Over the months and years that I struggled with depression and PTSD, I desperately wanted the array of antidepressants I was told to take to make me feel better. But at best they made me numb with a slew of side effects and ultimately a difficult withdrawal that took weeks.
Galynker wrote his book The Suicidal Crisis amidst a suicide rate that has steadily climbed despite wave after wave of new, designer antidepressants. Today suicide is the second leading cause of death in Canada for people aged 15 to 34.
“For one person who dies by suicide, 10 people attempt it, and 100 people think about it,” Galynker says.
Yet Galynker is cool on ketamine.
“I am somewhat skeptical,” he says. “A lot of its action comes from making people feel good as an opiate. I don’t know. I need to see the research. I withhold my judgment until I see more research.”
There is plenty of research into the failure of antidepressants and their link to suicide. Yet it doesn’t generate the same level of concern regulators like the B.C. College of Physicians and Surgeons have over low-dose ketamine.
Wei-Yi Song, past president of the Canadian Psychiatric Association, says he’s “quite aware” of the views of antidepressant critics like Healy.
Song stands by the efficacy of traditionally used antidepressants. But at the same time, he’s enthusiastic about ketamine’s ability to bring relief in a way that antidepressants don’t.

“Ketamine seems to be able to do that very rapidly. Within an hour. Typical antidepressants take two to four weeks,” Song says from his office in Victoria, B.C.
“Look, I can paddleboard to Vancouver, but it’ll probably take me a couple days,” he says. “Or I can take the Helijet in 40 minutes.” Ketamine treatment can be a mental-health Helijet option.
Yet B.C. has effectively grounded many potential flights to health at the same time there is a renaissance in the use of psychedelics to treat mental illness.
Ketamine is not the only non-traditional drug making inroads into mental health treatment.
MAPS — the Multidisciplinary Association for Psychedelic Studies — has spent years and millions of dollars investigating the safety and efficacy of MDMA, known colloquially as ecstasy, in treating PTSD. MAPS is on the verge of receiving FDA approval for MDMA use in the U.S. Approval in Canada is expected to follow.
And this fall, voters in Oregon will decide whether to legalize psilocybin for therapeutic use. It’s the active compound in psychedelic mushrooms.
Last year, a Vancouver advocate openly flouted Canada’s drug laws by advertising, making and selling microdose capsules of psilocybin to meet a growing demand from people influenced by the research of people like world-renowned mycologist Paul Stamets.
Stamets maintains that a regimen of microdoses of psilocybin, too small to have any psychedelic effect, produces a plethora of positive mental improvements. While there is a body of evidence supporting the idea, some of it anecdotal, it’s not surprising that drug companies haven’t conducted the same expensive and uncertain randomized double-blind clinical studies on psilocybin that’s done for every novel antidepressant. There’s simply no money in proving the efficacy of something anyone can grow in a shoebox.
So interested researchers are doing their own. Last fall, the University of British Columbia Behavioural Research Ethics Board lent its approval to a unique investigation backed by Stamets, MAPS Canada and others. The microdose study enrolled over 10,000 people through an iPhone app created by Quantified Citizen, a Vancouver-based company started by entrepreneurs who set out to disrupt the health research industry.
Eesmyal Santos-Brault is the CEO. He’s also on the board of MAPS Canada.
“MAPS in the U.S. is doing a great job with MDMA,” Santos-Brault says, “but if we take that same approach that they’ve been doing for all the other psychedelic compounds that are out there, it’s going to take way too long.”
The study relies on users anonymously logging their use of psychedelics and completing a series of check-ins through the app.
“It’s done in a rigorous way,” Santos-Brault says, “using validated measures, psychological scales where you’re doing cognitive tests, visual tests and hearing tests.”
Santos-Brault is reluctant to describe what the study has revealed so far (it needs more analysis and peer review). “All I can say is it’s promising and it’s very exciting and interesting.”
But while research enlisting 10,000 people who are using illegal psychedelics is seen as ethically OK, B.C. doctors like John Kristensen who want to use small doses of legal ketamine now risk losing their licences as a result of the college’s new rule.
“The lawyers are telling us to stay away from it,” Kristensen says. “But for the moment I’m ignoring it and carrying on. Like an abortion doctor in the old days when it was all taboo, because it’s morally impossible to not do this.”
Over the past several months I asked the B.C. College of Physicians and Surgeons a number of questions about the position it took in March — a position that was neither published, nor directly communicated to any of the doctors I spoke with. The college declined an interview request. It did respond to written questions. However, it wouldn’t describe the makeup of the committee that came up with the new rules, or provide any detail on the specialties of the committee members.
Just prior to this story being published, and after months of probing, the college finally posted a version of its position on its website. It reads nothing like the statement it came up with when I first began asking questions.
Essentially, the college now says ketamine is a dangerous drug with “potential serious side effects and other risks associated with its use.”
While the college acknowledges the relatively low doses involved in ketamine-assisted therapy don’t actually involve those risks, it is still holding fast to its order that psychiatrists, even those with years of experience, can’t be trusted to use it.
Ketamine, even in tiny doses, can now only be given “by a physician experienced in the administration of general anesthetics and airway management," the college has decreed. That effectively ends the ability of psychiatrists in B.C. to use a treatment that has proven effective in dealing with depressions and PTSD.
Kristensen says it amounts to responsible doctors being micromanaged.
“Why this paternalistic approach? I’m an experienced, longstanding physician,” he said. “You don’t need to hand-hold me. I don’t view the data [on the safety of ketamine] as being reckless. But the college is their own little kingdom.”
Kristensen’s defiance can be traced back to an experience three years ago. He was conducting a telemedicine appointment when the patient received a traumatic phone call.
“His son was found hanging,” Kristensen recalls. “But fortunately was cut down in time.” That man’s son — a 26-year-old lawyer in Toronto — had a history of depression.
Although Kristensen now lives in B.C., he works with his own son who’s a registered nurse in Ontario. Kristensen began treating the suicidal lawyer and says ketamine-assisted therapy ended the man’s suicidality.
“He was being treated by a University of Toronto psychiatrist who was aware of ketamine’s role, but she was not inclined to use it. I have psychiatrists call me out of the blue because they get word [that] I’m using ketamine. One said it’s a career breaker if you use ketamine. It’s going to impact your survival. Your standing.”
And how it might affect a doctor’s standing seems to depend on where they practice. There is no uniform application of rules across the country for using ketamine to assist in psychotherapy. P.E.I., Newfoundland and Labrador, New Brunswick, Saskatchewan and the N.W.T. have no position on its use at all.
Alberta seems to have found a compromise between Ontario and B.C., requiring any doctor who wants to use ketamine outside of a hospital setting to submit an application to a committee of their peers. But a spokesperson for the College of Physicians and Surgeons of Alberta says it has also struck a working group to look more closely at drugs like ketamine, and to determine how it might fall under new rules being developed that mirror B.C.’s policy about non-hospital surgical facilities.
“It’s got all of us a little frightened,” Kelowna psychiatrist Hanon says. “Because down in the States, some people have had their licences taken away.” He says patients are also paying a price.
“The college position is making it so that the natural course of disease is killing people, instead of allowing people who are capable of giving this life-saving treatment and giving it to people,” he says bluntly. “The college isn’t causing harm. They’re just not allowing the harm to be reduced.”
If the colleges are concerned about that image, they aren’t letting on. In a written response to questions, a spokesperson for the College of Physicians and Surgeons of B.C. disavows knowledge of any complaints.
“The college has not received any opposition from physicians on its position statement,” reads the unsigned email from its public affairs office.
“Even if there was opposition,” the college reply stated, “physicians are still obligated to comply with college standards and position statements.”
Rules are rules.
Josh McLarnon, a spokesperson for the Ontario college, provided some explanation for its review. Ketamine as a treatment “for anxiety, depression and PTSD is not yet fully supported by professional consensus or established clinical evidence,” he said in an emailed statement.
Any rule changes would involve “the expert input of any physicians who have had experience using ketamine-assisted therapy,” the statement said.
But Ontario psychiatrist Cornfield and some 50 physicians were told in direct correspondence from the college that they had just a three-week window to offer their comments to an opaque internal review looking at the future of ketamine. They feel that was hardly enough time to determine if there was a “professional consensus” about ketamine’s use.
The same statement from the Ontario college also rejects the idea that rules around ketamine as they currently exist effectively prohibit doctors from using it.
“As always, our expectation is that physicians only prescribe a drug if they have the knowledge, skill and judgment to do so safely and effectively.”
As it turns out, that’s what the doctors practising ketamine-assisted therapy want as well. ![]()
Read more: Health











Tyee Commenting Guidelines
Comments that violate guidelines risk being deleted, and violations may result in a temporary or permanent user ban. Maintain the spirit of good conversation to stay in the discussion.
*Please note The Tyee is not a forum for spreading misinformation about COVID-19, denying its existence or minimizing its risk to public health.
Do:
Do not: