




Just after Anthony Fauci, director of the U.S. National Institute of Allergy and Infectious Diseases, called the ebola outbreak "completely out of control," the government of Sierra Leone ordered its citizens to stay indoors for three days.
By any measure, ebola has turned one of the world's poorest geographies into a veritable hot zone.
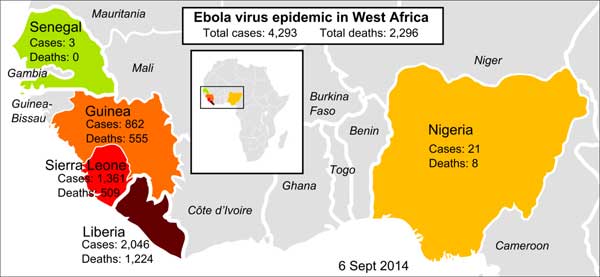
In Liberia, a poor nation of 4.5 million people, the epidemic is growing in an "essentially uncontrolled exponential manner."
Dr. Joanne Liu, international president of Médecins sans Frontières (MSF), now says "the world is losing the battle to contain it."
This nasty epidemic, which dispatches more than 50 per cent of its victims, should not be dismissed as some remote African horror story. The death toll is most recently about 2,300 and climbing.
It has highlighted key pest-fighting challenges for rich and poor alike, and offers some sobering insights on a number of other fronts, including globalization, bats, deforestation, unsustainable population growth and the limits to institutionalized global medicine.
The trouble with bigness
For starters, our technological society promises that only big organizations like the World Health Organization (WHO), a UN agency, can keep us safe from pandemics and other health tragedies.
But the poor of West Africa have learned differently. With dramatically slashed budgets and an epidemic unit employing just 52 people, the WHO has failed West Africa. Ebola just wasn't on their radar.
The outbreak began in 2013 in rural Guinea, but the WHO didn't declare an emergency until August 2014. At that point, the virus had already taken up residence in crowded urban slums where it could burn away for years like zebra mussels in the Great Lakes.
No real international response to the outbreak occurred until ebola starting infecting American aid workers. In Africa, it still takes a sick white man to alert people to the health realities of black men and women. When a Geneva-based global institution specifically designed to assist poor countries served by relatively few doctors can't do their job, then who can?
Large global institutions, from banks to corporations, tend to cultivate misery and inequality. Bigness doesn't care about local ecologies, let alone serving local needs. In many cases bigness just obliterates those realities and supports more bigness.
This is not to say that the world doesn't need top-notch scientific research and excellent public health agencies. It does. But these institutions should be nationally based, flexible, small and decentralized. They should be accountable to communities and not global economies.
Canada's modest but significant disease lab in Winnipeg, for example, contributed more initial expertise on the ebola outbreak than the WHO. But the Conservative government has cut the lab's budget to the bone.
Hospitals made it worse
The outbreak has also illustrated the folly of another centralized conceit: public health planning that puts hospitals at the centre of epidemic fighting.
In West Africa, hospitals were the first to be overwhelmed. Doctors and patients learned to fear them as sources and spreaders of infection. At one Sierra Leone hospital, 15 nurses bled out with ebola. The hospitals were the first to run out of gloves, syringes and protective gear.
In the end, hospitals did what they have done for centuries: they dutifully amplified the epidemic.
The lesson here is clear. Prabhjot Singh, a professor of international and public affairs at Columbia University, has emphasized the importance of training of community health workers to help trace suspected patients along with the infected in West Africa.
Effective pandemic or epidemic planning must focus on mobilizing and training local citizens. History explains why: a potent influenza or hemorrhagic virus such as ebola will shut down centralized healthcare and kill most first responders.
Carried by bats?
The viral strain now unsettling West Africa is Ebola Zaire. It first emerged in 1976 in central Africa and that's where subsequent outbreaks tended to cluster. But viral pandemonium has now exploded 2,500 kilometres away in West Africa, the distance between Halifax and Vancouver. Just how did that happen?
Bats, which serve as essential pollinators and insect controllers, and likely host five different strains of ebola that can melt human blood vessels, can easily migrate that distance.
Scientists suspect that virus spread from central to West Africa via bat migrations some time ago. The virus quietly took up residence in the forest until it spilled over into humans. Peppery bat soup is a popular delicacy in West Africa. The soup may also explain why many locals are immune to the disease.
Bats and humans share important similarities. Both mammals act as hosts for viruses, and both species are highly social and mobile. Only humans and bats can both form complicated social networks involving as many as a million individuals.
Much like waterfowl, the world's 1,000-plus bat species also harbor an extraordinary array of viruses. New studies show that small mammals including bats also host a "tremendous spectrum of relatives of human paramyxoviruses -- a family that contains the mumps virus, several different respiratory agents and the measles virus."
Scientists have made great progress breaking down and sequencing these viruses, but still know little about their ecology or why they emerge when they do. Bats, an ancient species, may even serve as unique viral mixers and carriers in nature. Disturbing and degrading bat habitat is a bit like opening Pandora's box.
A population gone viral
Ebola's rapid spread also owes much to West Africa's Malthusian human demographics. In 1950, most the region's poor (some 70 million) lived in rural areas. Today they are concentrated in chaotic urban slums. The region's 317 million will soon become a half billion by mid-century due to some of the world's highest fertility rates.
Ebola, of course, can be contained in isolated rural communities. More than a dozen previous outbreaks, which all appeared in remote areas, were stopped cold because the virus ran either out of hosts, or healthcare workers stopped human-to-human spread by changing local funeral practices.
But in Africa's crowded and hungry megacities, the virus has won untold entrepreneurial advantages. Tracing infected individuals in some of the world's fastest-growing slums is a nightmare. Even dogs are digging up corpses in shallow graves.
Michael Osterholm, the director of the Center for Infectious Disease Research and Policy at the University of Minnesota, says Africa has changed more than the original virus in the last 30 years. "If we just take a look at this current ebola outbreak, the virus hasn't changed. Africa has changed. We now have this virus in an urbanized population among people who travel far and wide."
But Osterholm might be wrong. Ebola Zaire seems to have shifted in many subtle ways. A recent paper in Science notes the virus's genome is changing so rapidly that current diagnostic tests may soon become outdated. Five of 50 researchers who co-authored the article died before the paper was published.
Epidemics are often graded by their R0, or reproductive number. A disease with less than one will die out quickly because there will be few secondary infections. Most ebola outbreaks in the past have recorded a R0 of 1.6 to 2.
In Liberia, the R0 appears to be three and rising. That means every infected individual will infect another three people. Researchers now predict that Liberia's ebola epidemic will experience "uninterrupted exponential growth."
Deadly deforestation
Epidemics always erupt in wounded geographies, and West Africa is no special case. The outbreak began in a remote corner of Guinea's denuded forests. In fact, West Africa has laid waste to its rich tropical rainforests in recent years.
The logging of forests, in turn, increases the likelihood that human and viral communities will collide. (Both HIV and SARS emerged from animals living in disturbed forests.) As humans dig for gold or plant cocoa in these tree-poor landscapes, the chance of coming into contact with ebola's suspected reservoirs, such as bats, chimps and antelope, increases. Healthy and diverse forests tend to keep viruses from spilling over into other populations. Monocultures, however, invite one calamity after another.
A 2012 study in the Onderstepoort Journal of Veterinary Research concluded "extensive deforestation and human activities in the depth of the forests may have promoted direct or indirect contact between humans and a natural reservoir of the virus."
In a more recent paper, Daniel Bausch, an ebola expert at Tulane University, adds that "large hemorrhagic fever virus outbreaks almost invariably occur in areas in which the economy and public health system have been decimated from years of civil conflict or failed development."
Bausch, who has travelled to the region for over a decade, has noted that the region keeps on getting poorer as its forests get smaller. Every time he drove from Guinea's capital city into the forest, he found a darker path: "The once-paved road got worse, the public services less, the prices higher, the forest thinner."
Peter Daszak, president of EcoHealth Alliance and a top disease ecologist, has repeatedly observed that human economic activities invariably drive disease emergence. "Pandemics are a product of our economic development -- they emerge when we domesticate new species, open up new trade routes, build roads into forests or expand air travel networks."
As a consequence, Daszak thinks that global mining, logging, transport and agricultural firms should post global public bonds to help fight pandemics. "Perhaps these industries should insure themselves against the rare but devastating pandemics their activities can sometimes cause. Additionally, health impact assessments, already used in many large development projects, could calculate and assess the pandemic risk of a project."
Problematic investors
Lastly, the epidemic has shed some light on the mercenary character of China's investments in Africa. The superpower has 20,000 nationals in Liberia, Sierra Leone and Guinea, largely there to plunder the region to support an unsustainable pathology at home: economic growth.
Roads and infrastructure built by the Chinese to transport goods are now highways for ebola, too. A handful of Chinese nationals have been quarantined.
To date, China has offered a paltry $5 million to combat the virus. It also sent along three teams of health care workers. In contrast, the United States has proposed nearly $100 million in assistance, with more than 100 scientists at the Centre for Disease Control on the case.
In West Africa, China is telling the world that their new world economic order behaves like a predatory hemorrhagic virus.
Meanwhile, ebola is telling the world that nothing supports viral spillover better than these technicians of a terrible epidemic: population growth, city-making, globalization and forest-clearing. ![]()
Read more: Health











Tyee Commenting Guidelines
Comments that violate guidelines risk being deleted, and violations may result in a temporary or permanent user ban. Maintain the spirit of good conversation to stay in the discussion.
*Please note The Tyee is not a forum for spreading misinformation about COVID-19, denying its existence or minimizing its risk to public health.
Do:
Do not: