




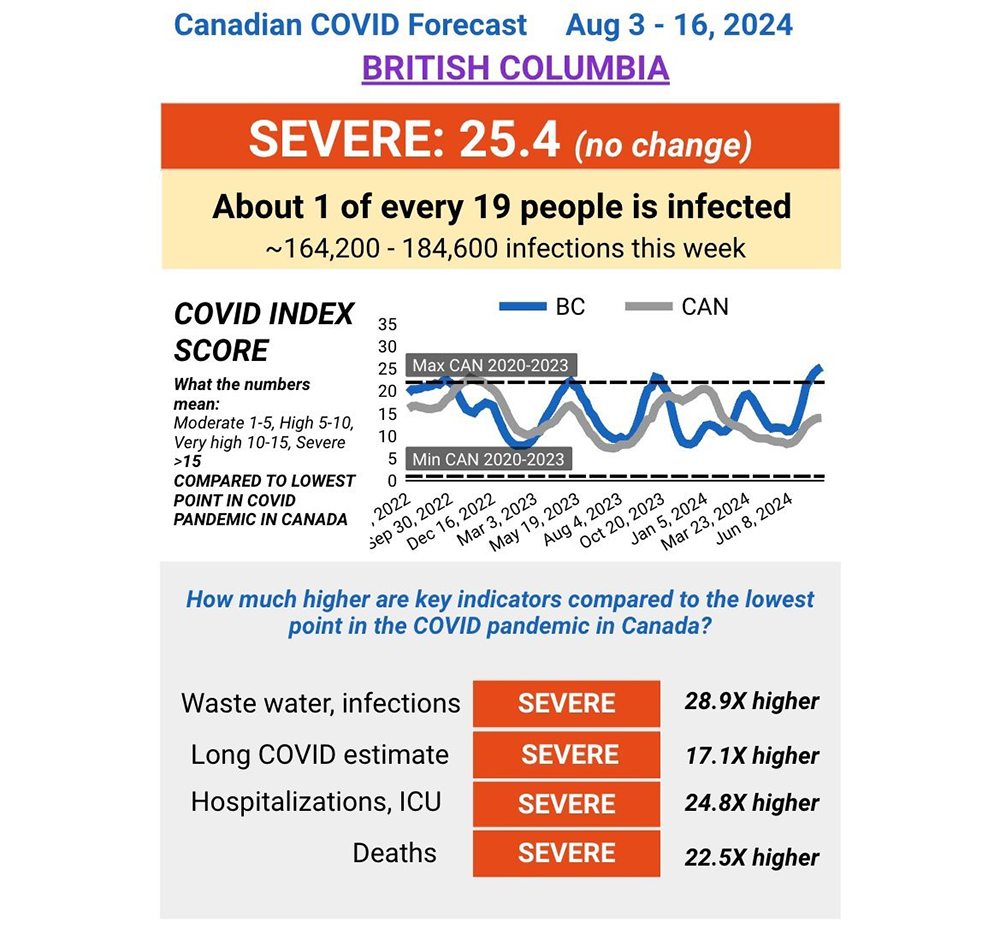
COVID is surging once again and, if you live in British Columbia, you probably already know someone sick with fever, chills and a sore throat.
As of mid-August, about one in every 19 British Columbians were enduring an infection, with or without symptoms.
Although the media routinely dismisses all COVID infections as an inconsequential nuisance, that’s not what the science says. The virus remains deadlier than the flu and repeated infections can radically change your health.
An important new Nature study, for example, has now proven that the spike protein of the virus can bind with a blood protein, fibrin, setting off a chain of blood clots resulting in chronic inflammation and brain damage. Fibrin can actually form a mesh impeding blood flow in arteries to multiple organs in the body.
Repeated studies show in the bluntest terms that the initial acute infection is only the tip of the iceberg. Even a mild bout of COVID can leave a legacy of blood clots, heart failure, diabetes, decreased brain function (see sidebar), long COVID (now affecting 400 million people worldwide) and immune damage that increasingly makes people more vulnerable to a plethora of infectious diseases and possibly cancers.
These problems can erupt three years after an infection and are especially prevalent in patients who’ve been hospitalized by COVID.
Which is why physical therapist and COVID specialist Dr. David Putrino emphasizes, “There is no such thing as a SARS-CoV-2 infection that does NOT have prolonged consequences.”
And yet the estimated daily level of infection in Canada now hovers around the highest points reached during the Omicron variant’s peaks in January 2022 and October 2023.
That’s the finding of University of Toronto infectious disease expert Tara Moriarty, whose team bases the latest COVID-19 Hazard Index on a combination of wastewater data and modelling. In a discursive and highly valuable X posting Moriarty adds “there's not a fresh vaccine in sight.” In fact, they are weeks away.
That means about one million infections are occurring every week and that this “severe” level of infection translates like clockwork into more than 1,000 deaths per week from COVID-19 in Canada based on five-week average trends. Ultimately these infections will result in more cases of long COVID in both younger and older populations.
While Moriarty’s estimates of COVID deaths are higher than provincial reports, the scientist asserts that her methods counteract chronic underreporting. Only 20 per cent of actual deaths from COVID are now reported, claims Moriarty.
There is more bad news: on an annual basis COVID infections still account for 20 times more deaths than influenza.
The data is not complete but this death toll likely made COVID the second or leading cause of death in the country last month.
According to Moriarty’s data, the number of COVID deaths per infection remain highest in Newfoundland, New Brunswick and Saskatchewan because they have older populations often compromised by serious medical conditions. They are also served by shrinking health resources.
Alberta, whose population is Canada’s youngest on average, claims the lowest infection fatality rate yet has already reported more than 700 COVID deaths this year. B.C. ranks somewhere in the middle.
These grim trends mirror COVID’s permutations south of the border. In the United States COVID infections hospitalized nearly five out of 100,000 Americans during the week of Aug. 4 to 10.
Dr. Ziyad Al-Aly, one of North America’s leading COVID researchers, notes that, “This crucial, yet lagging indicator hasn’t been this high since February 2024.” In addition, spotty U.S. data indicates that COVID has hospitalized twice as many people than the flu since October last year.
Rocking the system
Meanwhile Canada’s hospital emergency rooms, many already stretched before the pandemic, continue to open and close with troubling frequency across the country due to chronic staff shortages and sick workers.
With little surge capacity, the continued presence of highly infectious COVID variants continues to leave many health-care systems in shambles year after year.
According to Moriarty’s data, Canadian hospitals are now spending about $37 million dollars a day on COVID hospitalizations, which averaged more than 1,500 people a day two weeks ago.
Here’s some more damning math: “On average, since the beginning of Omicron, people needing hospitalization for COVID-19 account for 14 per cent of hospital bed capacity (seven per cent if you admit only half of people needing hospitalization).”
The resulting bed shortage has created a circular crisis, says Moriarty. “A constant annual seven-per-cent increase in hospital beds required for COVID-19, in a very low surge capacity environment with a serious health-care workforce labour shortage, can have profound upstream and downstream effects on health care and health.”
The evidence is everywhere. Five Interior B.C. emergency rooms closed over the long weekend. In the last week five rural hospitals temporarily closed in Alberta, including facilities in Swan Hills, Fairview and Rocky Mountain House. In Ontario some rural citizens refer to ER closures as an “epidemic.”
Dr. Alan Drummond, an Ontario rural physician, adds that the disruption of “emergency medicine delivery in Canada continues unabated as our political leaders fail to recognize and declare the obvious crisis that it is. They do nothing, they pray for divine intervention, they obfuscate, they lie through their teeth.”
‘A recipe for forever burn’
The subject of how to respond to a slow burn pandemic remains taboo because most public health officials have already declared the emergency over. They’ve also stopped collecting critical data. COVID-19 deaths in Canada are not reported in a readily publicly accessible fashion. And most of the media pretends that an immune-destabilizing virus that can harm the functioning of your organs including your brain has little more import than a benign cold.
As a consequence, authorities can’t now turn around and admit to the breadth of their mistake, let alone acknowledge the growing disorder in public health. Nor do they dare collect critical data documenting the scale of their errors including the relentless march of long COVID.
Meanwhile the virus continues to out-evolve our response and vaccines. Two months ago, when new COVID cases exceeded 100,000 a day in Japan, the research scientist Hiroshi Yasuda imagined the following discussion in a hospital.
Nurse: COVID hospitalizations are increasing again.
Doctor: I know.
N: Are we fighting an endless, losing battle against SARS-CoV-2?
D: No, you are wrong.
N: Oh, you have different ideas, doctor?
D: We are not even fighting.
N: [Nods in agreement.]
Richard Corsi, the noted U.S. indoor environmental engineer and creator of the Corsi-Rosenthal box, has summed up this predicament as a profound public health failure. “The general response to COVID-19 remains reactionary over precautionary. Wait until the fire gets hot and starts to burn rather than taking very simple steps to not fuel the fire in the first place. This is a recipe for forever non-containment, forever burn.”
He then points out: “The solution's been with us since day one of the pandemic. We've [generalized] just lacked the will, determination and grace to make it end. Reduce inhalation dose of virus-laden respiratory aerosol particles. It'll never end if we continue to run in the opposite direction, folks.”
The problem with running in the opposite direction, however, is that we increase the chances of landing in the arms of another COVID infection. And the reasons for avoiding such viral encounters just grow stronger by the sheer weight of evidence.
Why infection prevention still matters
Nobody sane really wants to play Russian roulette, but that’s how we should view every COVID infection. Although most people will get away with just an unpleasant biological disruption of daily life, others will take a bullet to their heart, brain, gut or immune system for reasons not fully understood.
No COVID infection is completely benign because each infection plays a role in deregulating the immune system. Even a mild infection, as one recent study noted, can increase “autoantibodies associated with rheumatic autoimmune diseases and diabetes in most individuals, regardless of vaccination status prior to infection.”
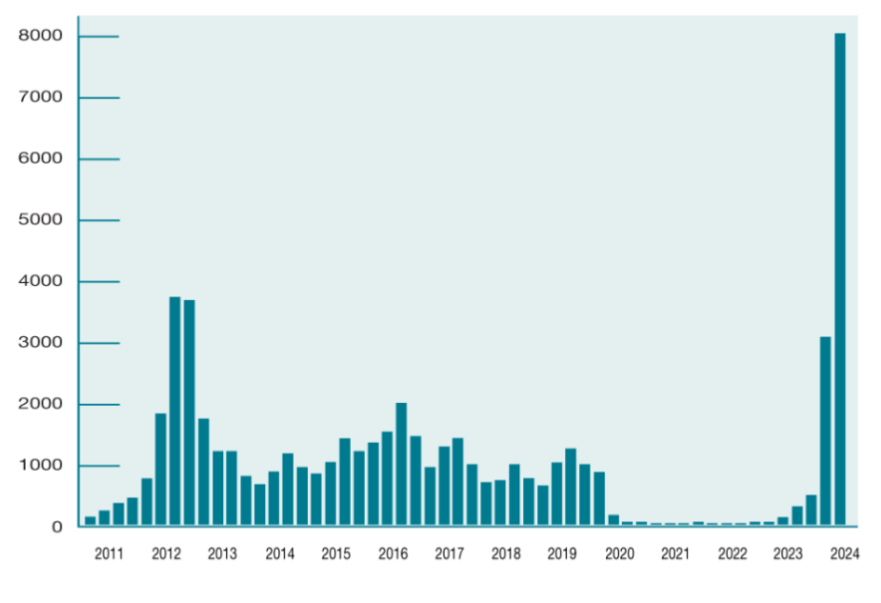
According to an increasing number of researchers, immune deregulation triggered by COVID probably plays a significant role in the dramatic global upticks in infectious diseases. The suspects include RSV, a variety of herpes viruses, whooping cough (now burning up the charts in Canada and England), scarlet fever, dengue fever, fungal infections and tuberculosis. Forty-four countries have now reported a 10-fold increase in the incidence of at least one of 13 infectious diseases compared to trends prior to the pandemic.
Although vaccine hesitancy, climate change and permissive travel have also played a role in this microbial wave, researchers strongly suspect that COVID’s disruption of the immune system has made it harder for many people to fight other infections.
Putrino, a COVID specialist at New York’s Icahn School of Medicine at Mount Sinai, recently explained the situation this way. “For the longest time we've told people that if you get an illness and you recover, it just makes you stronger. What we're seeing over and over again is that's not the case with COVID. Every time you get a COVID infection, your immune system seems to suffer.
“It's kind of like a boxer, every fight takes a little bit more out of them. And they're not getting stronger with every fight, they're not getting stronger with every hit that they take. Every single time there's an increased chance that something bad is going to happen to the immune system and I think that this influx of illness that we're seeing is related to that."
Another significant risk posed by playing Russian roulette with COVID infections is that each one could result in long COVID, which has sidelined 400 million people around the world at a cost of a trillion dollars. Some manifestations of long COVID include heart disease, diabetes, myalgic encephalomyelitis or chronic fatigue syndrome, and a raft of autoimmune diseases that may last a lifetime.
The risk increases with the severity of acute infection but the majority of long COVID sufferers have had a mild infection. The more times one is infected, the likelier the next infection will trigger a bout of long COVID. “Cumulatively, two infections yield a higher risk of long COVID than one infection and three infections yield a higher risk than two infections, explain researchers published in the journal Nature.
Here, then, is where we’ve arrived. We’ve entered a vicious cycle where more infections generate more COVID variants. The new variants have become more immune evasive. At the same time society has generally abandoned masks, testing and basic public health messages.
We could slow and suppress the cycle by facing the challenge squarely. For example, by cleaning dirty air the way we once tackled the disease-ridden spectre of cholera-infested water.
But public health officials are afraid to talk about clean air let alone the obvious: avoiding infection.
Beating back COVID requires hard work, communal wisdom and clear policies that markedly reduce the level of infection in society.
To date we have chosen viral denial, dirty air and a triumphant reign for long COVID. ![]()
Read more: Health, Coronavirus











Tyee Commenting Guidelines
Comments that violate guidelines risk being deleted, and violations may result in a temporary or permanent user ban. Maintain the spirit of good conversation to stay in the discussion and be patient with moderators. Comments are reviewed regularly but not in real time.
Do:
Do not: