



Ziyad Al-Aly, one of North America’s top COVID researchers, recently shared a critical message with the U.S. Senate.
“If we learn one thing from this pandemic, we must recognize that ‘pandemics disable people’ — that is acute infections can lead to chronic disabling disease.”
The epidemiologist knows what he is talking about, and his testimony to the U.S. Senate Committee on Health, Education, Labour and Pensions last month about the long COVID emergency deserves a broad audience.
He reminded the politicians that long COVID can affect the young and old. It doesn’t care what colour you are. It can follow severe as well as mild disease, and usually involves multiple organs.
It can disrupt the gut, fog and age the brain with Parkinson’s-like impact, disable the kidneys, damage the heart and cause chaos in the immune system. The post-viral condition has more than 200 symptoms. There is no treatment yet.
One of the afflicted eloquently described long COVID this way: "It is a constant deluge of pain that slowly strips you of everything you used to be by taking away everything you used to do — daily exercise, going out more nights than not, seeing friends, attending concerts.”
Al-Aly told the senators, “We don’t go through an earthquake without dealing with its aftermath. We cannot live through the biggest pandemic of our lives without dealing with the aftermath. That aftermath is long COVID. We must address the challenge of long COVID.”
Millions in Canada and US have long COVID
Al-Aly knows this aftermath well because he and his team at Washington University in St. Louis documented the first characteristics of long COVID and did the most widely cited research on the condition. The Tyee has highlighted his important work repeatedly.
Al-Aly testified that the condition of long COVID now afflicts at least 20 million Americans. Their disability represents an economic toll of $3.7 trillion in terms of lost productivity and lost lives. That’s a loss equal to the 2008 recession.
Canada shares this great burden. According to a recent Statistics Canada survey, more than two million Canadians reported suffering from the symptoms of long COVID as of June. That’s seven per cent of the adult population. More than half report no improvement in their condition over time. More than one in five Canadians battling long COVID on average took 24 days off from work or school.
Al-Aly also highlighted one of the key findings of that little-cited Canadian survey and even shared a graph from the study showing that reinfections heighten the risk of long COVID.
“Even if people managed to emerge unscathed after the first infection, they may get long COVID after reinfection,” warned Al-Aly.
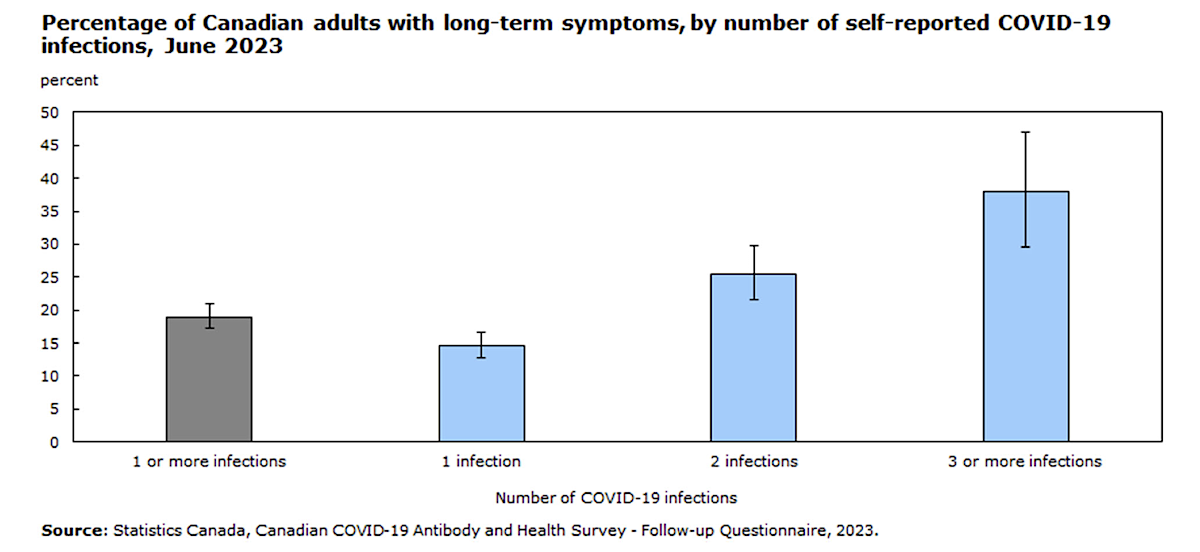
The Statistics Canada survey found that Canadians reporting two COVID-19 infections were 1.7 times more likely to report prolonged symptoms of long COVID than those reporting only one infection.
Those who had experienced three or more COVID infections (and that’s become most of us) were 2.6 times more likely to develop long COVID.
A U.S. program found similar results: “Ten per cent of people with one infection had long COVID, compared to 20 per cent of those with two or more infections.”
Yet somehow the reality isn’t getting through to most people. As Al-Aly reminded the senators, “The risks of getting long COVID after reinfection are not known to the general public.”
Given the evolution of COVID, the arrival of new variants and the sustained rate of hospitalizations around the world, the pandemic is seeding more and more chronic disease.
“Between low rate of recovery and new cases from reinfection and breakthrough infection, long COVID will continue to increase until we find better ways to prevent it and treat it,” testified the doctor.
How to cut down on long COVID
There remains only one way to prevent long COVID, said Al-Aly, and that is to avoid infection. (He wore a mask while giving his testimony.)
And that requires a sustained multi-pronged approach by public health officials.
It requires better and variant-proof vaccines that block infection for several years. It requires complete transparency on vaccine side-effects because they do exist.

“We must recognize vaccine injury,” Al-Aly said. “We must understand how it happens and how to mitigate it. Understanding vaccine injury will not only help us produce safer vaccines, but it can also offer insights into the mechanisms of long COVID.”
Preventing long COVID requires ventilation and air filtration systems in schools and hospitals to stop the spread of COVID. Bad air is an eminently fixable problem.
“We did an amazing job proofing our buildings against earthquakes that happen once every few decades or few centuries,” Al-Aly said. “Why don’t we proof our buildings against the hazards of airborne pathogens? We can and should do this.”
It requires sustained research and investment in antiviral treatments for a health burden as great as cancer and heart disease.
“We developed vaccines at warp speed. We are doing trials for long COVID at snail speed.”
“We urgently need large-scale trials to test a broad array of repurposed drugs and development of novel drugs to treat long COVID.”
Al-Aly then told the senators that COVID is not unique in causing chronic illness.
Pandemics have long tails because their viral and bacterial authors often have long-term crippling effects.
The virus responsible for the Spanish flu set the stage for a wave of Parkinson’s disease decades later. People born during that pandemic had a threefold increased risk of later developing Parkinson’s.
The Epstein-Barr virus, once called the kissing disease, can lead to cancer, diabetes or multiple sclerosis decades later. An innocent flu-like infection can later erupt into a debilitating condition known as myalgic encephalomyelitis/chronic fatigue syndrome. And so on.
“The idea that a virus that produces acute infections can also cause chronic disease is not new. We just ignored it for 100 years,” said Al-Aly.
He then explained that the current research effort on long COVID did not match the scale and the urgency of a growing problem as the pandemic continues. “Research effort must be commensurate with the burden of disease caused by these infections. And it should be executed with a sense of urgency.”
He recommended the establishment of an institute for infection-associated chronic illnesses with a budget of at least $1 billion per year.
He ended his testimony with this observation: “Because pandemics will continue to happen (and their frequency will likely be higher in the 21st century than in the 20th century), and because pandemics will likely produce in their wake droves of people with chronic disease and disability, understanding how infections cause chronic illnesses should also be a cornerstone of pandemic preparedness and resilience.”
Bernie Sanders, chair of the U.S. Senate committee, obviously was listening.
In a recent editorial, Sanders wrote, “We cannot turn our backs on the millions of Americans who continue to struggle with long COVID-19 — or the millions more who may contract it in the future. The time to act is now.”
Canadians might want to ask who with power is paying attention to the plague of long COVID in this country. ![]()
Read more: Health, Politics, Coronavirus











Tyee Commenting Guidelines
Comments that violate guidelines risk being deleted, and violations may result in a temporary or permanent user ban. Maintain the spirit of good conversation to stay in the discussion and be patient with moderators. Comments are reviewed regularly but not in real time.
Do:
Do not: